
- Видео 95
- Просмотров 1 186 901
Elias Hanna
США
Добавлен 20 янв 2021
Cardiovascular hemodynamics
Coronary catheter techniques
Coronary angiographic techniques
Cardiology tips
Coronary catheter techniques
Coronary angiographic techniques
Cardiology tips
Guide dissection: cases and management
+ Review general dissection classification and management at 24:07 and at ruclips.net/video/eGdfIk73cds/видео.html
0:00 Case 1 and guide dissection causes
03:17 Proper AL1 engagement technique
05:09 General approach to guide dissection. Stent proximally vs distally. Proximal stenting most important and sometimes enough
10:06 Approach if you don’t have a wire across
12:20 and 13:05 How to wire in case of dissection
14:24 and 24:04 IVUS features of false lumen/intramural hematoma
15:24 Advanced tips for when you fail to wire true lumen (parallel wire, STRAW)
17:37 Role of IIb/IIIa antagonists
19:11 stenting tips
20:51 Case 1 distal stenting: crush stent through Guideliner
24:57 General dissection cla...
0:00 Case 1 and guide dissection causes
03:17 Proper AL1 engagement technique
05:09 General approach to guide dissection. Stent proximally vs distally. Proximal stenting most important and sometimes enough
10:06 Approach if you don’t have a wire across
12:20 and 13:05 How to wire in case of dissection
14:24 and 24:04 IVUS features of false lumen/intramural hematoma
15:24 Advanced tips for when you fail to wire true lumen (parallel wire, STRAW)
17:37 Role of IIb/IIIa antagonists
19:11 stenting tips
20:51 Case 1 distal stenting: crush stent through Guideliner
24:57 General dissection cla...
Просмотров: 480
Видео


Interesting coronary angiograms and decision-making -3
Просмотров 4,8 тыс.28 дней назад
0:00 Case 1 RCA engagement caveat 1 04:30 Case 2 RCA engagement caveat 2 07:12 Case 3 RCA engagement caveat 3 11:12 Question regarding bicuspid aortic valve 11:41 Case 4: LIMA side branch: causes ischemia? 21:03 Case 5: Coronary microfistulae? Thebesian? 30:51 Case 6: LV hemodynamics- LV support? 39:30 Case 7 44:04 Case 8: left main atheroma or something else? IVUS images 47:07 Case 9: STEMI pl...

Heavy coronary thrombus
Просмотров 3,1 тыс.Месяц назад
0:00 Case, definition and outline 01:19 The 4 major techniques of treating heavy coronary thrombus: technical tips and data 06:45 Stenting heavy thrombus: how? Timing? Stenting risks? 08:55 Laser, Angiojet 10:23 Additional case 12:27 IVUS images of thrombus. Plaque erosion 14:18 Additional Case. Cerebral stent retriever technique and steps 18:34 Summary: 4 major techniques, 1 stenting idea, and...

Cardiac arrest
Просмотров 4 тыс.Месяц назад
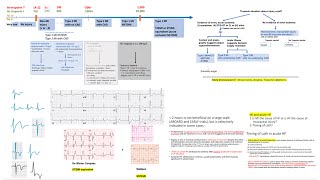
0:00 Brief on types of cardiac arrest and survival. Brief on PEA (02:30) 04:15 Classification of cardiac arrest based on post arrest ECG- Probability of acute CAD and chronic CAD 07:33 Cath in patients with no ST elevation on post-arrest ECG? COACT and TOMAHAWK- Why? 12:29 Cath in patients with ST elevation on post arrest ECG? 3 factors to account for 14:30 Importance of timing of post-arrest E...

Cardiogenic shock: tips and updates
Просмотров 6 тыс.2 месяца назад
00:25 Classification of the 2 big types and 4 subtypes of cardiogenic shock, and which one need immediate cath- Pitfalls of NSTEMI-shock and HF-shock 07:13 Support devices. Pitfalls of IABP SHOCK II and ECLS shock trials vs DanGer 09:38 DanGer shock trial key features and interpretation 14:58 U shape curve of benefit 19:35 IMPORTANT summary slide: when to cath and when to support based on the 4...

NSTEMI part 2. Pharmacotherapy: antiplatelets, anticoagulants, other therapies
Просмотров 4,5 тыс.2 месяца назад
01:10 1-Other therapies 01:10 β-blocker: acute, long term, low EF, normal EF 10:14 ACE-I 13:21 Aldosterone antagonist 16:01 Entresto and SGLT-2 inhibitors 20:08 Summary slide 23:22 2-Antiplatelet therapy 23:22 Clopidogrel vs prasugrel vs ticagrelor: differences? which one to use? Factors to consider? Should we preload? 36:58 De-escalation from potent P2Y12 inhibitors DAPT to clopidogrel DAPT at...
NSTEMI
Просмотров 9 тыс.3 месяца назад
Review Chapter 1 of my book, my 3 STEMI talks and my ECG ST elevation talks, as they complement this lecture. ruclips.net/video/wtBIG8a8Wbg/видео.html ruclips.net/video/zbu1y_AEQrY/видео.html 0:00 4 Types of myocardial injuries. Diagnostic tips and tricks 07:24 General management of non-MI injury and type 2 MI 07:52 Type 2 MI vs type 1 overlap and difficult cases 12:02 Hs-troponin T and I 12:02...

Access complications and management
Просмотров 8 тыс.3 месяца назад
Focused on femoral access complications. 0:00 Femoral access, ultrasound and anatomy tips 09:29 High stick and closure devices 11:57 Closure devices pitfalls-Board questions 13:15 Groin hematoma. Limited role of femo-stop device 16:17 Hypotension during or after PCI: differential diagnosis 17:58 Retroperitoneal bleeding diagnosis and management 20:40 Avoid CT scan acutely 24:15 Hazards of acute...

Left main trifurcation strategies
Просмотров 4,7 тыс.4 месяца назад
This talk complements my other bifurcation talks and is an exercise that further enhances understanding of bifurcation techniques. 0:00 General concepts and classification 04:20 General technical approach with drawings. When and how to Double stent? Triple stent? Which techniques? 17:00 Case illustrations with drawings: case 1 21:07 Case 2
Coronary perforation
Просмотров 5 тыс.5 месяцев назад
0:00 Types of coronary perforation (large vessel vs small vessel) Ellis classification 02:51 Approach to management of each of the 2 big types/algorithms 06:58 Fat embolization 09:09 General coils types and steps- Microcatheter compatibility. 12:20 Pushable coils deployment 15:42 Detachable coils deployment videos 21:39 Case illustration 23:52 Large vessel perforation- Covered stents- How to ad...
Isolated ostial LAD or ostial LCx stenting
Просмотров 9 тыс.5 месяцев назад
0:00 2 major approaches 01:32 Nail the ostium strategy. Pitfalls 03:43 Troubleshooting 06:59 Crossover stenting into LM. Provisional steps 10:13 Ostial LCx compromise with LAD stenting. Risk factors and management 14:29 Same 2 strategies for isolated ostial LCx stenosis 16:55 Avoid touching uninvolved branch and kissing balloon if no compromise 20:27 Avoid Szabo technique 22:06 Data and cases
Interesting coronary angiograms -2
Просмотров 10 тыс.6 месяцев назад
For more advanced cases, jump to 08:26 0:00 Cases 1 and 2 08:26 Cases 3-4 13:23 Collaterals formation, grades and timelines (also 47:31) 14:51 Case 5 21:45 Case 6. Dead AV groove conduit 25:22 Case 7 (with ECG discussion) 33:16 Case 8 (with ECG discussion, also 46:00) 45:18 LVgram comment 47:31 Collateral classification and timing 49:23 Case 9 54:53 How to do complex LM case with no support-Imp...
ECG QRS abnormalities- Part 2
Просмотров 3,5 тыс.6 месяцев назад
0:00 Case 1 01:37 RVH criteria. Importance of axis shift (different from LVH) 04:53 Case 2 05:47 and 09:35 RVH-RBBB overlap. How to diagnose RVH in RBBB (07:37 No right axis in pure RBBB) 10:32 LVH and LBBB vs RVH and RBBB 11:30 Case 3 13:20 Right atrial enlargement criteria 14:31 Case 4 18:16 Secondary ST-T abnormalities in RVH/RBBB vs LVH/LBBB 20:15 Case 5. Lung disease pattern vs RVH vs ante...
ECG QRS abnormalities- Part 1
Просмотров 6 тыс.7 месяцев назад
01:27 ECG 1- Goldberger ECG 05:31 ECG 2 07:21 ECG 3 07:40 LVH voltage criteria 12:21 ECG 4 13:16 LVH-LBBB overlap. LVH with incomplete vs complete LBBB. Progression of hypertensive and myocardial disease (14:13). Features of incomplete LBBB (15:22) 16:42 Clinical significance of LBBB. When does it suggest cardiomyopathy 18:04 Additional LVH ideas: left axis deviation? Voltage criteria in younge...
Hemodynamic cases- part 2
Просмотров 3,2 тыс.7 месяцев назад
0:00 Case 1 (RA) 03:44 Cases 2 and 3 (RA) 06:43 Case 4 (MS; discussion of gradient vs MVA, echo vs cath) 15:21 Hybrid approach of MVA calculation, combining echo and cath 16:42 Case 5 (MS) 18:25 Case 6 20:61 Case 7 23:14 how to simultaneously measure LV-aortic pressures 24:51 Technical pitfalls, damping 29:28 Summary: 4 steps to ensure proper measurements, with summary slide (01:08:45) 31:30 Ca...
Bifurcation Left main part 2: case studies (2-stent techniques)
Просмотров 6 тыс.8 месяцев назад
Bifurcation Left main part 2: case studies (2-stent techniques)
Constriction vs Myocardial disease: practice cases and tracings. Misunderstood concepts.Board review
Просмотров 2,7 тыс.9 месяцев назад
Constriction vs Myocardial disease: practice cases and tracings. Misunderstood concepts.Board review
Bifurcation left main stenting- Elias Hanna
Просмотров 10 тыс.9 месяцев назад
Bifurcation left main stenting- Elias Hanna
MI with plaque disruption on IVUS/OCT but stenosis less than 50%: should you stent?
Просмотров 3,2 тыс.9 месяцев назад
MI with plaque disruption on IVUS/OCT but stenosis less than 50%: should you stent?
IVUS/OCT stent guidance, pre- and post-stenting
Просмотров 8 тыс.9 месяцев назад
IVUS/OCT stent guidance, pre- and post-stenting
Radial loops- Difficult radial, subclavian and aortic anatomy: step-by-step, cases, perforation
Просмотров 6 тыс.10 месяцев назад
Radial loops- Difficult radial, subclavian and aortic anatomy: step-by-step, cases, perforation
Left+right coronary engagement for general fellows: step-by-step tips, diagrams, caveats (5 for RCA)
Просмотров 16 тыс.10 месяцев назад
Left right coronary engagement for general fellows: step-by-step tips, diagrams, caveats (5 for RCA)
Left EBU/CLS guides manipulations, radial and femoral +Ikari L +Key tips in left coronary engagement
Просмотров 14 тыс.11 месяцев назад
Left EBU/CLS guides manipulations, radial and femoral Ikari L Key tips in left coronary engagement
Amplatz L guide manipulations/videos- Other RCA guides and tips- The 5 RCA engagement caveats- Hanna
Просмотров 8 тыс.11 месяцев назад
Amplatz L guide manipulations/videos- Other RCA guides and tips- The 5 RCA engagement caveats- Hanna
Vein graft PCI: Focus on distal embolic protection-how, when, pitfalls, troubleshooting- Elias Hanna
Просмотров 4,7 тыс.Год назад
Vein graft PCI: Focus on distal embolic protection-how, when, pitfalls, troubleshooting- Elias Hanna
Axillary balloon pump (+Impella): step-by-step access, exchange, closure, complications- Elias Hanna
Просмотров 3,3 тыс.Год назад
Axillary balloon pump ( Impella): step-by-step access, exchange, closure, complications- Elias Hanna
Balloon pump: hemodynamics, troubleshooting, technical tips- Elias Hanna
Просмотров 14 тыс.Год назад
Balloon pump: hemodynamics, troubleshooting, technical tips- Elias Hanna
SCAD cases and discussion- Air embolism cases Elias Hanna
Просмотров 6 тыс.Год назад
SCAD cases and discussion- Air embolism cases Elias Hanna
❤
AL catheters , especially for the RCA, especially 7 and 8 French , are WEAPONS. I remember being a first/ second year fellow back in ‘80 - ‘81. If Dr. S. , the Chief, had to use a 8 French AL 2 for even the LCA, it was going to be a long day in the lab and the Surgeon was going to be busy! The catheters in those days were a piece of work. Ah, the “ good old days”.
❤
Thank you so much Dr Hanna❤
Thank you 😊
Great presentation as usual sir, thanks a lot.
Amazing lectures and a great book on hemodynamics. There can be a difference between PCWP and LV if there is some constriction at AV groove or Mitral stenosis. With a LV-PCWP trace alone can we diagnose CCP? Another point - IVC pressure is not affected by respiration while SVC is affected because IVC is mainly abdominal and not thoracic ?
Thank you very much
Thanks a lot
Thank you sir❤
Deeply Thanks
Awesome Lecture , Thanks a lot
Great Thanks Sir
Thank you Dr. Hanna. How about manual aspiration thrombectomy through guideliner or other type of aspiration catheter, instead of Penumbra System?
Can i get the pdf of this legendary lecture
Thank you for your amazing talk~~
Excellent
Very interesting viedo again
Thank you sir for one more great lecture as always.
Great vid ❤
Huge thanks to you. The work you put in throughout your videos and textbook helps us immensely.
Thank you sir for one more clinical pearls
Thank you for sharing. I have one question for TAP, which wire do you recemended to use for final POT ?
We use the MB wire for final POT. You may review a video animation of the TAP steps I have under Bifurcation LM part 1: ruclips.net/video/IU43KJYIvu8/видео.html
@@eliashanna8248 Thank you Sir
Thank you. This is very helpful 😊😊
Thanks a Million Times
Thank you our great prof thank you a million
Thanks my mentor
I am a cardiology fellow and i've watched lots of videos throughout my medical training. this is one of the best overview videos of any topic I've ever seen, thank you!
Elias, you r really doing good work, by helping Cardiology residents throughout the world, and thereby saving thousands of lives.
Exactly!!!
You are the teacher of all around the world's interventionalists. Thanks Dr. Hanna....
Excellent as usual
thanks a lot for simplifying and make it easily understandable for an undergraduate like me ❤️
Top talk Dr. Hanna. We are waiting for a lecture about laser. Thank you
excellent !!
Thans Dr Hanna for this excellent talk. requesting you for a talk(s) on CTO PCI, which is a complex area.
Thank you Doctor Hanna, very informative and in depth as always.
Great presentation, highly appreciated!
Dr Hanna thank you for your excellent lectures.When you give intracoronary eptifibatide, what dose do you use and how do you mix the intracoronary bolus, Thank you
Thank you! And great question. We use the same bolus dose that would be used intravenously, which is what was used in all trials of IC GPI. I administer each bolus via a 10 ml syringe, sometimes 2 syringes mixed with blood. For eptifibatide, we use the standard 2 boluses of 180 mcg/kg/bolus, given 10 min apart (or 1 dose if GFR<50); and for tirofiban, we use the standard one dose. This is followed by the standard IV infusion for up to 24 hrs. Eptifibatide solution is acidic, and there is a hypothetical concern about microvascular injury using it directly in the coronary; so, if possible, try to buffer the bolus by mixing a bit of blood in the syringe (blood aspirated via the guide/Tuohy). One study has buffered 10 ml of Eptifibatide with 2 ml of bicarb 8.4%, but that is somewhat less practical.
Thank you from Australia. Amazing talk as usual. My only thought is that if using a strong suction like Penumbra attached to your Tuohy, a threaded/screw end type valve for a stronger seal. I would worry a spring loaded valve might entrain air and also reduce the suction effect.
Thank you. You are correct. There is a concern about vacuum suctioning when connecting Penumbra suction to Tuohy/Guideliner, which creates air and air embolism. That is why, after this maneuver, it is important to remove the Guideliner from the body while on negative suction, then back bleed the Tuohy vigorously (passively initially, to get potential air out).
Dear Dr Hanna, thank you so much for the great lecture.. im a great fan of your lectures and have always learnt alot from your lectures.. I have a question: You mentioned the idea of avoiding stenting and marinating the patient with glycoprotein 2b/3a inhibitors for ~24hours in case the heavy thrombus persists.. what if the heavy thrombus burden persists even after repeat angio? The cerebral stent retreiver isnt availabe in our cath labs in the UK, so what would be your strategy in case of persistent heavy thrombus burden on the repeat angio? Many thanks
Thank you! IT is likely that one of the 4 essential techniques will work, especially the local tpa. IF none worked and marinating the pt did not work either, consider laser if you have it. Another technique that is somewhat similar and more widely available than stent retriever is to deploy a Filter or Spider wire distal to the clot. Then pull the Filter wire and try to trap the clot and pull it in the guide. There is, however, a concern about clot dislodgement and aortic/cerebral embolization doing this; stent retriever is safer in that regard, as it integrates into the thrombus.
As usual....brilliant lecture.... Please shed some light on thrombus trapping by direct stenting and what about avoiding pre and post dilatation in case of thrombus containing lesion...???
Thank you! I will give you the same reply as below: The idea of direct stenting does not apply to heavy thrombus. As I describe, you do not want to stent in the midst of very heavy thrombus, as you have a high risk of macro and micro embolization from cheese crater effect (rather than trapping the thrombus, you squeezed it through the stent cells; remember the stent has open cells). Also, significant risk of stent thrombosis, esp if you aggravate distal flow. The cerebral stent retriever concept is different: it is s a slow self-expanding stent (no balloon) that is pulled out. In milder thrombus burden (thrombus <2 vessel diameters, esp <1/2 vessel diamters), direct stenting may have some merit via reducing the overall manipulations and potentially reducing distal emboli and improving reperfusion, based on 5 small trials (A meta-analysis of randomized controlled trials of conventional stenting versus direct stenting in patients with acute myocardial infarction.J Invasive Cardiol 2015;27:405). However, direct stenting necessitates that the artery is not totally occluded and has flow, whether at baseline or after wiring; if it is totally occluded, you have to get some flow before direct stenting, via thrombectomy (which is not recommended if thrombus burden not high, class III) or lesion dottering with deflated balloon. Overall, I do not believe it has a major role, and a more modern meta-analysis did not show a benefit (European Heart Journal 2018: 39: 2472-2479). It has risks in some subsets and several limitations. This was more relevant in the early 2010s, when thrombectomy was routine and when we could do thrombectomy followed by stenting. But TOTAL trial showed the hazard of routine thrombectomy and it is now class III in the guidelines. As an extension of those ideas, post-stenting is what should be limited in STEMI to reduce embolization and cheese crater effect.
Thank you for the valuable inputs......
Thanks for your presentation may you add The ECG of inferior STEMI heavy thrombus for purposes of early recognition
Thank you Dr. Hanna for the great taeching. Just one question: Why should we exactly use a dual lumen catheter for i.c. II.b/IIIa or i.c. lysis rather a standard microcatheter. Thanks for your answer.
You may use a standard microcatheter, but you would have to pull out the wire to inject the drugs. A dual lumen catheter allows you to maintain distal wire access and also has the advantage of being monorail system. It is a Monorail system that allows you to maintain distal wire access, while you inject the drugs via the OTW port
Very helpful and nice talk dear Dr. Hanna. What do you think about directly stenting the lesion with thrombus and avoid ballooning it to prevent distal embolization?
Thank you! The idea of direct stenting does not apply to heavy thrombus. As I describe, you do not want to stent in the midst of very heavy thrombus, as you have a high risk of macro and micro embolization from cheese crater effect (rather than trapping the thrombus, you squeeze it through the stent cells; remember the stent has open cells). Also, significant risk of stent thrombosis, esp if you aggravate distal flow. The cerebral stent retriever concept is different: it is s a slow self-expanding stent (no balloon) that is pulled out. In milder thrombus burden (thrombus <2 vessel diameters, esp <1/2 vessel diamters), direct stenting may have some merit via reducing the overall manipulations and potentially reducing distal emboli and improving reperfusion, based on 5 small trials (A meta-analysis of randomized controlled trials of conventional stenting versus direct stenting in patients with acute myocardial infarction.J Invasive Cardiol 2015;27:405). However, direct stenting necessitates that the artery is not totally occluded and has flow, whether at baseline or after wiring; if it is totally occluded, you have to get some flow before direct stenting, via thrombectomy (which is not recommended if thrombus burden not high, class III) or lesion dottering with deflated balloon. Overall, I do not believe it has a major role, and a more modern meta-analysis did not show a benefit (European Heart Journal 2018: 39: 2472-2479). It has risks in some subsets and several limitations. This was more relevant in the early 2010s, when thrombectomy was routine and when we could do thrombectomy followed by stenting. But TOTAL trial showed the hazard of routine thrombectomy and it is now class III in the guidelines. As an extension of those ideas, post-stenting is what should be limited in STEMI to reduce embolization and cheese crater effect.
@@eliashanna8248thank you for the detailed answer. I am glad to have your book and be able to hear your voice and communicate with you on youtube. Greetings from Germany. ❤
This is a phenomenal talk as usual Dr. Hanna. I miss working with you so much
Ahmed, the best interventional fellow ever :). We all miss you!!
I don’t like performing LV gram in acute MI shock patients. Adding more volume worsens the shock. An ECHO is easier to perform and can answer all the Qs.
You are god sent!
Great
Sir please upload a video about ffr, ep study
Excellent lecture sir 🙏